We hadn’t found a new class of antibiotics in decades:
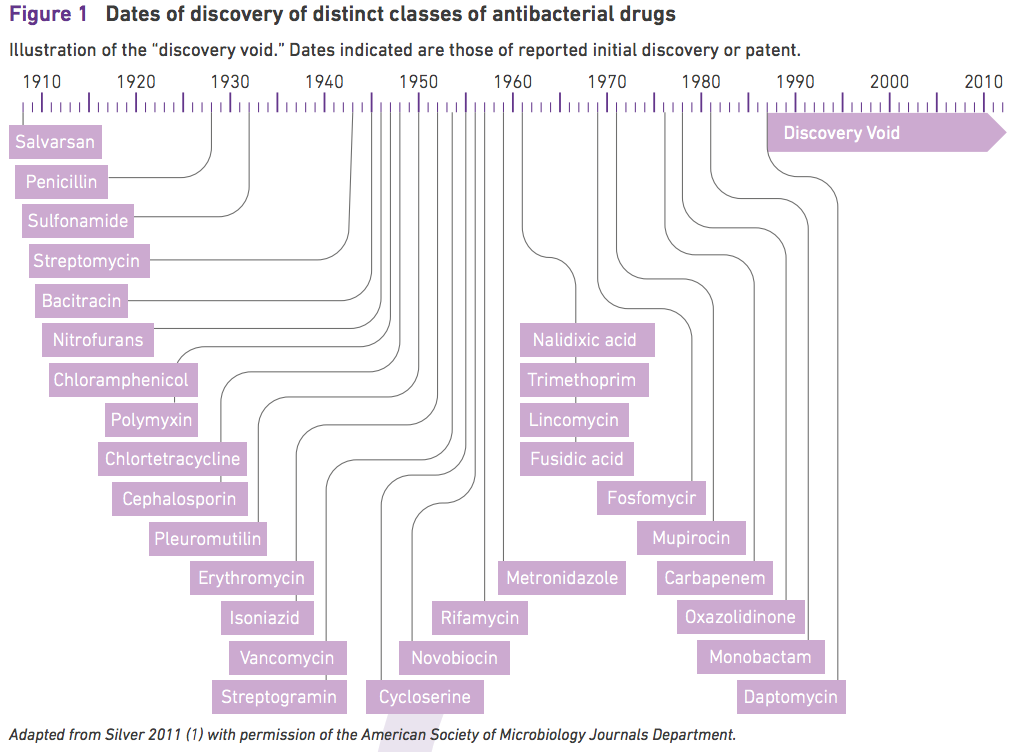
Which is what makes this news so exciting:
A new antibiotic – the first in nearly 30 years – has been discovered by scientists who claim it appears to be as good, or even better, than many existing drugs with the potential to work against a broad range of fatal infections such as pneumonia and tuberculosis. Laboratory tests have shown the new antibiotic, called teixobactin, can kill some bacteria as quickly as established antibiotics and can cure laboratory mice suffering from bacterial infections with no toxic side-effects.
How teixobactin was discovered is likely to be more important than the drug itself. Heidi Ledford explains:
Many of the most successful antibiotics were found in the mid-twentieth century by scientists who trawled microbial communities for bacteria capable of killing their brethren. But the researchers missed the type that produces teixobactin, Eleftheria terrae, plus many other potential candidates — known collectively as microbial ‘dark matter’ — because of their reluctance to adapt to life on a petri dish.
[Kim] Lewis and his Northeastern colleague Slava Epstein discovered E. terrae’s potential with a device they call the iChip. It works by sorting individual bacterial cells harvested from soil into single chambers. The device is then buried back in the ground. Several molecules in that environment are able to diffuse into the iChip, allowing the bacteria to thrive in a more natural setting than a petri dish. Typically, only about 1% of microbes in a soil sample are able to grow in the lab. The iChip expands that fraction to 50%.
Ed Yong is enthusiastic about iChip:
Teixobactin is a fish; the iChip is the rod. Having the rod guarantees that we’ll get more fish—and we desperately need more.
Bacteria have been fighting each other for billions of years before we arrived, so environmental microbes are a rich source of potential new antibiotics. The problem is that 99 percent of them won’t grow in lab conditions. So, why not bring the environment into the lab?
That’s what the iChip does.
Sarah Zhang takes a closer look at teixobactin:
As for teixobactin, it’s promising, but don’t expect it to be a game-changer all by itself. It works by inhibiting the growth the cell walls in bacteria, a mechanism that is difficult (but not impossible!) for bacteria to evolve resistance against. But that also means teixobactin only works against bacteria without another membrane around those cell walls. That includes bacteria like MRSA and TB, but not other worrisome ones like Klebsiella and E. coli, which have evolved a lot of resistance to existing antibiotics.
Teixobactin will still have to be tested in humans for safety and efficacy. It will have to be easy to synthesize in large quantities and ideally ingestible rather than only injectable. There are many characteristics of a good antibiotic beyond just being able to kill bacteria. Don’t expectteixobactin to be available for several years, and that’s assuming it pans out.
Arielle Duhaime-Ross puts the discovery in context:
Henry Chambers, an infectious disease researcher at the University of California, San Francisco, who didn’t participate in the study, thinks the researchers’ new approach is interesting. But the fact that the antibiotic isn’t effective against most Gram-negative bacteria is slightly disappointing. “There are now plenty of drugs for infections caused by Gram-positive,” he said, “and the more pressing need is for resistant Gram-negatives.”
Chambers also cautions against getting too excited about the idea of a new antibiotic. It’s “too early to get excited for yet to be proven clinical utility,” Chambers says. And even if the drug is approved for human use, it won’t solve the current problem of widespread antibiotic resistance — a problem that stems from overuse in both medicine and food production. “If an antibiotic is used enough, resistance ultimately will emerge.” For example, although it took 40 years for resistance to develop against vancomycin — another antibiotic that works in a similar way — resistance did eventually occur. Still, if teixobactin is approved for human use in a few years, that will be good news, Chambers says. “New potent and effective antibiotics belonging to a novel class are welcome, even for Gram-positives.”
The researchers believe it will take decades for bacteria to become resistant to teixobactin:
While widespread resistance to new drugs typically takes anywhere from weeks to years, Lewis anticipates that resistance to teixobacitn may take decades to develop, citing vancomycin, a drug often used to treat MRSA infections, and considered a drug of last resort—one typically saved unless there are no other options. Developed in England in the 1960s, vancomycin, which also targets a bacterial cell-wall polymer rather than a protein, only began to encounter resistance in the 1990s. “So that gives us an idea of how long it will take for resistance to develop to teixobactin,” he says. “It should take more than 30 years.”
Judy Stone is skeptical of such claims:
The researchers are too glowingly optimistic about the likelihood of resistance emerging, I believe. In fact, the compound is being touted as “resistant to resistance” based on lab testing. Bacteria are always smarter than the people who develop and use them. While it may have taken 30+ years for Vancomycin resistance to develop, in part that is likely because we didn’t use that much of it until the last decade. …
My biggest concern, should Teixobactin make it to market, is that it will be squandered as every other good new antibiotic has been, and so resistance will rapidly emerge as the drug is overused. I have particularly been disappointed to see this with the other novel antibiotics developed during my career—Linezolid (Pfizer) and Daptomycin. I see both marketed irresponsibly (including promoting use to Social Service case workers) because they are convenient to use. Medicare has not been willing to pay for home IV antibiotics, so many of us use Daptomycin, which can be given once-daily in an outpatient clinic, so that our patients won’t have to go to a nursing home to receive antibiotics. As a result, we’re creating bacteria resistant to one of our few remaining effective antibiotics. Similarly, Linezolid is wasted for convenience, since it can be given orally; it has also been promoted for inappropriate uses, as treating colonization in wounds or in nursing home patients, rather than infection.
