A NYT investigative report finds that “there was a moment in the spring when the longest and deadliest Ebola outbreak in history might have been stopped”, but failures of communication among health officials in West Africa enabled it to spiral out of control:
A two-month investigation by The New York Times into this largely unexamined period discovered that the W.H.O. and the Guinean health ministry documented in March that a handful of people had recently died or been sick with Ebola-like symptoms across the border in Sierra Leone. But information about two of those possible infections never reached senior health officials and the team investigating suspected cases in Sierra Leone. As a result, it was not until late May, after more than two months of unchecked contagion, that Sierra Leone recorded its first confirmed cases. The chain of illnesses and deaths links those cases directly to the two cases that were never followed up in March.
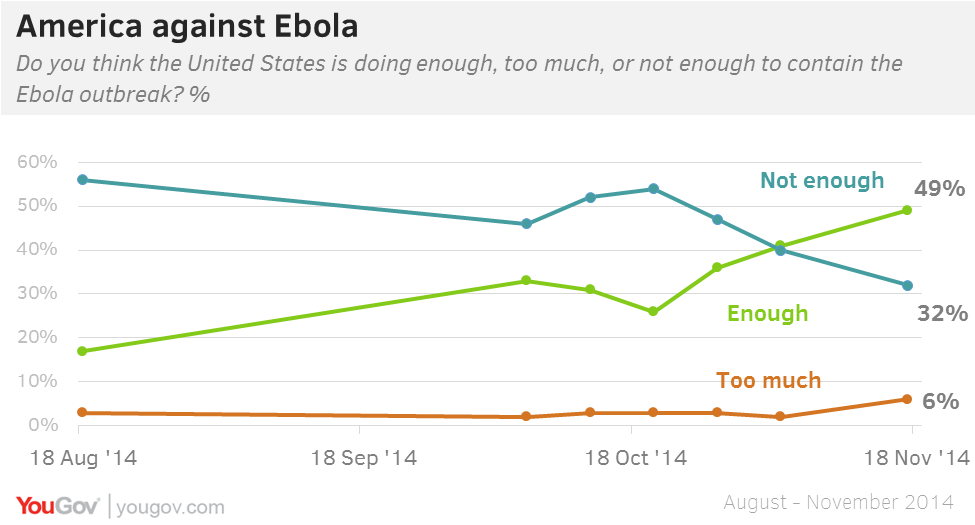
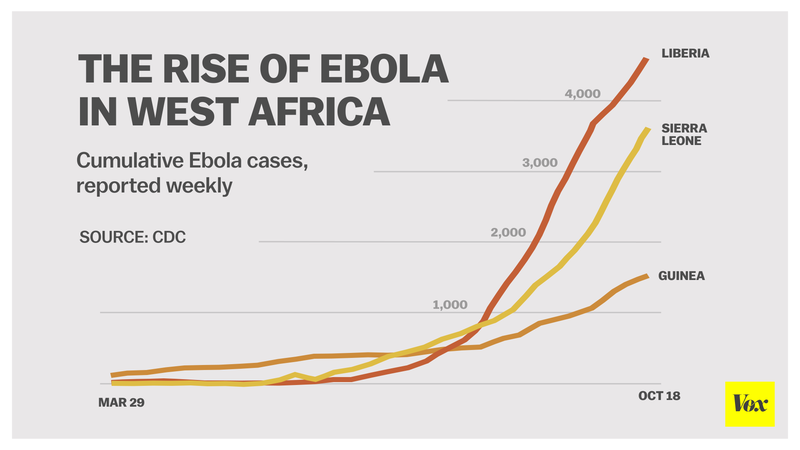
Since then, West African authorities and international organizations have followed a steep learning curve, Alexandra Ossola writes, but containing the outbreak (which the WHO reports has now infected over 20,000 people) remains a daunting task:
The WHO and others have disseminated information about proper burials to dissuade families from conducting funeral practices that may cause further infection, and they have been pretty effective. But there are still too many risky burials; Sierra Leone, which still has the highest number of cases, did not meet its December 1 goal of safe burials for 70 percent of victims.
… There are signs that these countries are fighting Ebola more effectively, [CDC spokesperson Kristen] Nordlund said, but challenges remain. Health care workers are still struggling to contain Ebola’s spread in cities like Freetown, Sierra Leone. When people move across borders between countries with high infection rates, tracking down the people who may have come into contact with a patient becomes extremely challenging. Some hospitals still don’t have enough beds to safely treat infected patients, Nordlund said, and not all regions have sufficient number of medical personnel to do the necessary follow-up with those who may have been exposed.
Meanwhile, a group of scientists has put forth a theory as to how the outbreak made the jump from animals to its first human victim, a two-year-old boy from the remote Guinean village of Meliandou:
Reporting in the journal EMBO Molecular Medicine, scientists led by Fabian Leendertz at Berlin’s Robert Koch Institute delved into the circumstances surrounding this first fatality. The finger of suspicion points at insectivorous free-tailed bats — Mops condylurus in Latin — that lived in a hollow tree 50 metres (yards) from the boy’s home, they said. “The close proximity of a large colony of free-tailed bats… provided opportunity for infection. Children regularly caught and played with bats in this tree,” the team said after an exhaustive four-week probe carried out in April.
In other Ebola news, another returning health worker has carried the disease home with her, this time in the UK. Scottish nurse Pauline Cafferkey was diagnosed yesterday after returning from Sierra Leone, where she had been volunteering along with other NHS health workers:
Ms Cafferkey, who had been working with Save the Children in Sierra Leone, arrived in Glasgow on a British Airways flight on Sunday but was placed in an isolation unit at Gartnavel Hospital on Monday morning after becoming feverish. [Scotland’s First Minister Nicola] Sturgeon told journalists that as a precaution, Health Protection Scotland has traced and contacted, or left messages with, 63 of the 70 other passengers who were on the same flight from London to Glasgow as the patient.