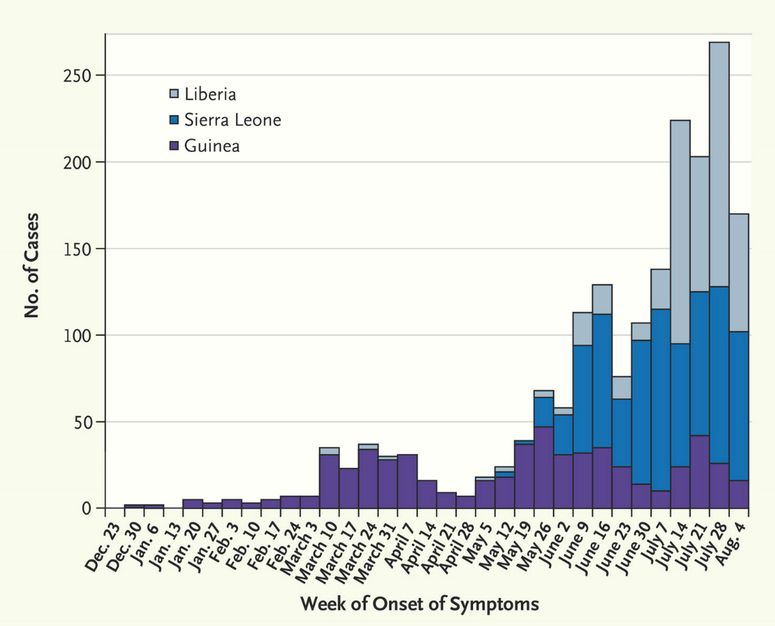
Julia Belluz flags an eye-opening chart on the growing severity of the Ebola crisis:

The situation is dire in West Point, a Liberian slum:
Tens of thousands of people are trapped in a slum in Liberia’s capital, Monrovia, after officials put the neighborhood under strict quarantine to prevent the spread of Ebola. Clashes broke out on Wednesday, as riot police and soldiers attempted to barricade angry residents. Days earlier, locals had raided a holding center for suspected Ebola patients, pulling out mattresses covered in blood, which could spread the disease.
Per Liljas provides more details:
On Saturday, a health center was looted and Ebola patients sent running, after a rumor spread that infected people were being brought in from other parts of the country. Others refused to believe the disease existed. “There is no Ebola,” some protesters attacking the clinic shouted. “There is a high level of disbelief in the government in West Point,” Sanj Srikanthan, the International Rescue Committee’s emergency response director in Liberia, tells TIME. “The government has made a concerted effort to reach out to community leaders, youth groups and churches with the message that the only way to contain the disease is to understand it. But some people still believe Ebola is a conspiracy, and those people we need to reach.”
Raphael Frankfurter is unsurprised “that aggressive, opaque public health measures are met with suspicion, resistance, and anger”:
In public health, the emphasis on “harmful behaviors” arising from ignorance fails to acknowledge the complex socioeconomic factors and structural conditions that can lead to poor health.
In the wake of the first Ebola cases in Guinea, the Guinean government and later the Sierra Leonean government launched a massive campaign to persuade people not to hunt and consume bushmeat, which is thought to carry Ebola. Though well-intentioned, these campaigns did not adequately consider that malnutrition is widespread in rural West Africa, and villages in which the population heavily relies on bushmeat are often healthier—in our experience, they even have significantly lower rates of malnourishment. It wasn’t just an issue of people “not knowing” not to eat fruit bats and gorillas—bushmeat was their only source of protein. Continuing to eat it can be understood as a rational decision based on a risk assessment—malnutrition will likely always lead to more deaths in West Africa than an Ebola outbreak.
But I’ve also observed through four years of fieldwork in Sierra Leone that public health interventions that rely on the passive reception of “medical facts” by target communities and that hinge on getting “them” to think like “us,” are simply ineffective. To health workers, taking patients home to die in surrounded by their families, to be collectively buried and remembered in their villages might be considered “irrational” or “contributing to the spread of the disease.” But these practices also allow for a kind of solidarity and resilience in the face of capricious, cruel disease.
Liljas emphasizes the desperation of aid workers as they continue to battle the ebola outbreak in West Africa with limited support from overstretched international organizations:
[T]he biggest unmet need is for additional well-trained health workers. Professionals on the ground are exhausted, and several hundred have died in part because of a lack of training. MSF and other organizations are stretched to breaking point, some of them because of their involvement in other crises. USAID, for example, is responding to four humanitarian crises at the same time: South Sudan, Syria, Iraq and the Ebola outbreak. It must also weigh up whether to put people at risk.
David Francis details how the virus is also endangering the region’s fragile economy:
The outbreak comes at an inopportune time for the region. Prior to the outbreak, the Nigerian economy was being celebrated as the largest in Africa, with a GDP of $510 billion, compared with second-place South Africa, with a GDP of $353 billion. Sierra Leone is attempting to draw foreign investment to its diamond industry and saw its GDP grow 20.1 percent from 2012 to 2013. In 2013, Guinea’s GDP grew a modest 2 percent.
All of these positives are now overshadowed by the bleak prediction of Ebola’s ramifications in the region. The World Bank estimates that Guinea’s GDP will shrink between 3.5 and 4.5 percent this year as Ebola roils the agricultural sector and discourages regional trade. Liberia’s finance minister, Amara Konneh, lowered the country’s GDP estimates by 5.9 percent because of the outbreak. Bismarck Rewane, CEO of the Financial Derivatives Company, a Lagos-based financial advisory and research firm that manages $18 million in assets, told CNBC Africa on Monday, Aug. 18, that Nigeria could lose at least $3.5 billion of its $510 billion GDP. Moody’s has already warned that the virus could hinder the region’s energy sector.